
Every day, Dr. Leslie Miller of Fairfield thinks about selling her practice to a hospital health system.
“Everybody who is in this environment thinks every day of throwing in the towel and joining a hospital,” said Miller, a sole practitioner in primary care for 20 years. “The business side is the problem,” she said, referring to expensive and time-consuming requirements of medical insurance and government regulations.
Dr. Khuram Ghumman took the unusual route of working in a hospital system first, then going into private primary care practice because he objects to the “corporatization” of health care. He said conflicts of interest can arise if an owner and its employed physicians have different objectives. “I wanted to be responsible to my patients,” Ghumman said.
Nationally and in Connecticut, hospital systems and private businesses are increasingly buying private medical practices and taking over their business operations. American Medical Association statistics show just 46% of physicians owned their own practices in 2018, down from 75% in 1983.
In Connecticut, hospital health systems range from large groups, like Yale New Haven Health Services and Hartford Health Care, to systems owned by one hospital, like UConn Health. They are all non-profit except Prospect CT Medical Foundation, a for-profit company which owns Waterbury, Manchester and Rockville hospitals.
There are other medical systems as well, such as ProHealth Physicians, owned by Optum, a division of the company that owns the insurer United Healthcare. Private equity firms have also invested in medical practices, including orthopedic and emergency medicine groups.
An area of active practice acquisition is primary care, at a time when demand for preventive health care is rising along with an aging population.
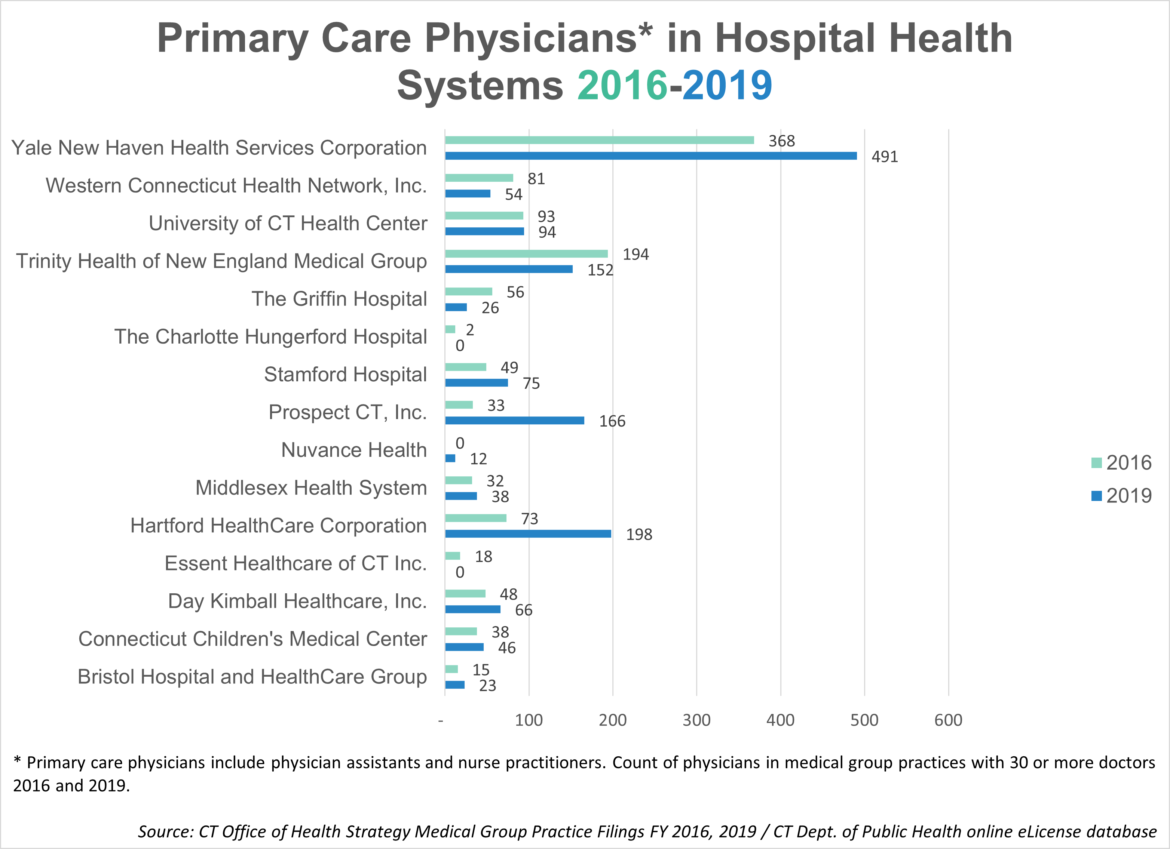
Primary care practitioners in hospital systems’ practices of 30 or more doctors increased from 1,100 in 2016 to 1,441 in 2019 – a 31% rise, according to data from the state Office of Health Strategy (OHS). At Yale they rose from 368 to 491, (33%); Hartford Health Care from 73 to 198, (171%); and Middlesex Health System from 32 to 38, (19%). The acquisitions include doctors, physician assistants and nurse practitioners.
Hospital health systems say that they provide improved, streamlined and coordinated care because primary care providers and specialists can work together and have easier access to patients’ medical records.
But studies report that acquisitions are driving up the cost of health care and doctors lose the freedom to manage their own scheduling.

Cloe Poisson Photo.
Dr. Khuram Ghumman directs patient Carlos Padilla where to look as he checks his eyes during an annual physical.
Ghumman, who practices in East Granby, said he spends an hour with patients on physical exams and a half-hour on follow-up visits. “I just want to pose the question to physicians: who do you work for?” he asked.
Miller said she prefers her autonomy, is comfortable with the way she runs her practice, likes the intimacy of it and the ability to give patients the choice of going to a solo practitioner.
Dr. Andrew Wormser, a New Haven internist affiliated with Yale’s Northeast Medical Group, said “there is some lack of autonomy,” but added “they still give us enough that we can practice the way we want to.”
Wormser is part of the Connecticut Medical Group, established by a group of physicians in the 1990s to pool resources. He explained that a more complex regulatory climate and the resultant need for investment in electronic medical records prompted the sale of the practice to Yale in 2012. Under the arrangement, the 31 physicians are contractors, not employees, but Yale owns the business. “The hassles of running the office are no longer there, which is a lot,” Wormser said.
C-HIT requested interviews with officials of Yale New Haven Health, Hartford Health Care, Trinity Health of New England and the Connecticut Hospital Association (CHA); none were granted. CHA provided a statement, saying: “Partnerships between hospitals and health systems and physician practices preserve and expand access to care, support care improvement and often enable new value-based care arrangements.”
Isaac Kastenbaum, vice president of the nonprofit Primary Care Development Corporation, said that primary care practices are particularly ripe for acquisition or merger.
“What’s required of a primary care practice today is very different from what was required 20 years ago,” he said.
Regulatory and insurance requirements necessitate “an amount of staffing, technical expertise and capital that independent practices just can’t raise by themselves for the most part, or it’s very difficult,” said Kastenbaum, whose organization provides loans and technical assistance to primary care providers.
Financial losses and costs connected to practicing medicine during the COVID-19 pandemic has exacerbated pressures on private practitioners, said Dr. Gary Price, president of the national Physicians Foundation and a Clinton plastic surgeon. “COVID made a bad situation much, much worse,” he said.
Independent practices are also threatened because young physicians don’t want to run businesses. They want to be employees focused on practicing medicine and having a balanced lifestyle, said Victoria Veltri, OHS executive director.
State’s Effort: Improve Health Care, Control Costs
The OHS is spearheading a project to increase spending on primary care in an effort to improve health, control long-term health costs, improve access to and quality of preventive care, and address social determinants of health. A 2019 report on 29 states put Connecticut at the bottom of primary care spending, defined as physician care in offices and outpatient settings. The report by the Patient-Centered Primary Care Collaborative and the Robert Graham Center found Connecticut spent 3.5% of its health care spending on such primary care between 2011 and 2016.
The state’s goal is for primary care to account for 10% of overall health care spending by 2025. “A better-resourced primary care system can create a better outcome for patients and lower overall health care spending over time,” Veltri said.
 She said that there is growing interest in “team-based care” to address a range of patient needs. That means that primary care practices could include, for example, social workers and pharmacists in addition to medical practitioners.
She said that there is growing interest in “team-based care” to address a range of patient needs. That means that primary care practices could include, for example, social workers and pharmacists in addition to medical practitioners.
“That’s how primary care is evolving,” she said. “We’re trying to keep people healthy. We’re trying to intercede early in health care issues and address things like social determinants of health, social drivers of health,” she said.
This is occurring at a time when shortages of primary care physicians are projected through 2033, new doctors are turning to more lucrative specialties to help pay for medical school debt, and Connecticut is having a difficult time attracting doctors. According to an Association of American Medical Colleges report using 2018 data, Connecticut ranked 41st in the country in retaining doctors who either attended medical school or trained as residents in the state.
Meanwhile, a proposed law would give the state more oversight over medical practice acquisitions by allowing state review for acquisitions of any size, instead of the current minimum of eight physicians. It would also remove the existing presumption of approval.
“You could be a Yale or Hartford Health Care or Nuvance and could acquire a practice of seven, another practice of seven, another practice of four, another practice of five” and it isn’t subject to state review, Veltri said, explaining that lack of review prevents opportunities to limit increases in health care costs. Costs for patients and the Medicare program are higher in hospital-owned practices, according to the Physicians Advocacy Institute.
Hospitals and physicians opposed the proposal at a recent legislative hearing. Dr. Jeffrey Cohen, head of clinical services for Hartford Health Care, said his system acquired 30 practices with less than eight physicians in the past three years, adding that there are “few medical practices with eight.” He warned that independent doctors could go out of business waiting for the reviews to be conducted.
In a statement, the Connecticut State Medical Society said that many small group medical practices are barely surviving, but said, “it is not in the purview of the legislature to dictate under what circumstances physicians may decide to sell their practices.” The medical society said that the state should focus instead on issues that burden independent physicians, such as insurance coverage contracts that don’t allow doctors to negotiate rates, exclusionary policies and high malpractice rates.
Cloe Poisson Photo.
Dr. Khuram Ghumman in his office in East Granby.
Managing His Own Practice
Ghumman said he is spared many administrative tasks because of his practice’s structure, with seven physicians, five nurse practitioners, a physician’s assistant, and sufficient office staff to handle business operations. “If you have systems in place that are working for you and your patients, you can still do without having to be a part of a large corporate system,” he said.
He compared the current health care landscape to when most independent pharmacies were pushed out of business by competition from chains, eliminating the choice of going to a small pharmacy.
“If you lose the ability to make choices in health care, that’s a sad day for everyone—not just doctors, but patients,” he said.
I have practiced independently in a 1-2 doctor practice for 44 years. I have saved a lot of lives and helped improve a lot more. My staff has been as high as 8 and as low as 2. We always put patients first and love our patients like family. Lately our practice has been mostly primary care for women. The landscape has changed radically in the national push for universal care. Hospital systems and large groups forming mega entities is clearly antitrust. BUT starting with Obama, antitrust has been ignored. The goal is to form 2-3 large systems/state gobbling up everything site unimpeded. The government figures that it will be easier to deal with 2-3 entities per state than thousands of doctor practice when they take over. In the meanwhile, the big entities suck the life out of smaller practices until they die. Sad for patients in the end.
i highly doubt breaking up the large hospital systems through antitrust laws will magically make smaller practices financially viable. if you’ve truly been an independent practitioner for 44 years, i’m sure you understand that the rising administrative costs are the real burden – hence why the smaller ones are selling out to the bigger ones in the first place.
your theory that the big bad democrats are going after small private practices because they’re somehow the only thing standing in the way of that darn socialist national healthcare is certainly amusing though…