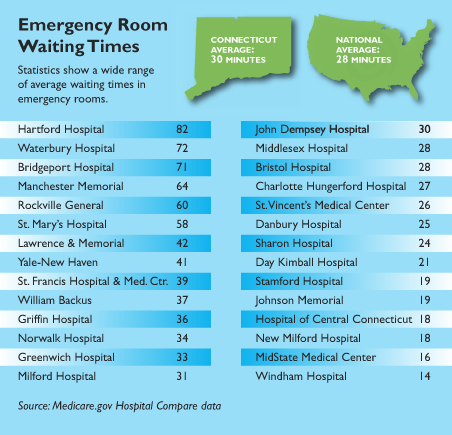
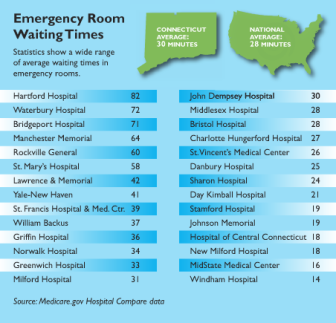
In more than half of Connecticut’s emergency rooms, the waiting time to see a health-care provider exceeds the national average of 28 minutes – a problem that experts say could get worse, as thousands more residents obtain health insurance.
WebKazoo Graphic
The average wait can stretch to an hour or more at Rockville General, Manchester Memorial, Bridgeport, Waterbury and Hartford hospitals, according to a C-HIT review of federal data. The statewide average waiting time is 30 minutes.
The longest wait time is at Hartford Hospital, where patients were not seen for 82 minutes, on average; the shortest wait of 14 minutes is at Windham Hospital, the data compiled by the Centers for Medicare & Medicaid Services (CMS) through 2012 show. Officials at Hartford and Bridgeport hospitals claim shorter wait times than the federal data.
Hospitals have taken some steps to improve their wait times, at a time when emergency departments have seen an increase in patients. But, experts say that the task is only going to get tougher, as the Affordable Care Act (ACA) will expand the pool of eligible Medicaid recipients seeking care by at least 15 million nationally.
With a shortage of primary care physicians or those who won’t accept new patients, ER visits are bound to increase in Connecticut when the ACA takes effect in 2014, said Dr. Gregory Shangold, medical director of Windham’s emergency department.
“Insurance does not equal access to care,’’ he said. “The emergency department is society’s safety net.”
Efforts To Reduce Waiting Times
Officials at several hospitals say they are streamlining their ER operations to shorten waits for walk-in patients. They note that patients who arrive by ambulances or with life-threatening conditions are seen right away. Some hospitals post their waiting times on their websites, so people will know what to expect.
At Hartford Hospital – where officials say the median door-to-provider time of 37 minutes is a better measure of its wait time than CMS’ calculation – a “quick track’’ room frees up ER beds while patients wait for lab results. Bridgeport Hospital, with an average ER wait time of 71 minutes, recently added two physicians to handle its 81,000 annual ER visits.
“The seven-hour wait went out with the tide,’’ said Dr. Rockman Ferrigno, chairman of emergency medicine at Bridgeport Hospital. “We’re all challenged by the same thing: how to provide quick, quality, compassionate care.”
The focus on ER waiting times comes as use is rising in Connecticut and around the country.
From 1997 to 2007, ER visits increased nationally by 23 percent, the Journal of the American Medical Association reports. The National Center for Health Statistics reports that mean ER waits also climbed – from 46.5 minutes in 2003 to 58.1 minutes in 2009.
In Connecticut, total ER visits increased by 55,000, or 3.2 percent, from 2011 to 2012, according to the state Office of Health Care Access annual hospital report. The six hospitals with the highest total ER volume were Yale-New Haven, Hartford, The Hospital of Central Connecticut, Middlesex, MidState and Lawrence & Memorial hospitals.
More patients are using the ER because the U.S. population is aging and the number of primary care physicians has not kept up with the demands of sicker people, said Dr. Robert C. Solomon of the American College of Emergency Physicians.
“More people are going to the emergency department because…no one gets turned away,” Solomon, an ER doctor in Pittsburgh, said.
Dr. David Goldwag, medical director of Waterbury Hospital’s emergency department, said his hospital is concerned about its average 72-minute waiting time and is studying its entire ER operation to reduce long waits.
Ferrigno said a better measure than Bridgeport’s 71-minute average is the 45-minute median time for a patient to see a physician in his ER. Triage has been speeded up, and he said patients waiting for lab results are now placed in a monitored waiting room to free up ER beds.
Since Hartford is the only Level 1 trauma center in Greater Hartford, it may have longer waits than other hospitals, said Rebecca Stewart, spokeswoman for Hartford Hospital.
The other Level 1 trauma center in Connecticut, Yale-New Haven Hospital, has an average ER wait of 41 minutes, according to the data.
Dr. Jeffrey A. Finkelstein, chief of emergency medicine at Hartford Hospital and The Hospital of Central Connecticut, said Hartford is shortening its ER waits through several steps, including having a fast track for people with minor ailments.
The new Quick Track or Q Track program is also working well, he said, as other patients are monitored in a “results-pending area with 14 comfortable chairs, coffee and a big-screen TV.’’ Q Track is novel, he said, because “it speeds the care for everyone.”
Elaina Schultz of Tolland said she has used Rockville’s ER often when her husband, Chuck, has fallen or had low-blood sugar, and that he is usually seen in five to 10 minutes, rather than in the 60-minute average reported in federal data. Sometimes, though, he’s waited up to eight hours for lab results or to be admitted, she said.
“It’s almost like they’ve forgotten you’re there,’’ she said. “But if every cubicle is filled and patients are out in the hall, you have to use your common sense and realize they’ll help you when they can.”
At Windham, the average wait has been cut to 14 minutes by streamlining triage and moving patients to rooms quickly, Shangold said.
Hospitals are also working to cut down on the waiting time to be admitted as inpatients from ERs.
“Unfortunately, sometimes you have to put people in hallways in the ED,’’ Shangold said. “It’s not ideal.”
That practice is known as “boarding,” which Solomon said has become widespread around the country.
Stamford Hospital uses a “bed ahead” approach to speed up admissions from the ER. A doctor starts the hunt for a regular hospital bed as soon as a condition that will require admission, such as a hip fracture, is diagnosed, said Dr. Jayson Podber, chairman of Stamford’s department of emergency medicine.
Podber said his ER has also reduced its average waiting time to 19 minutes by having a doctor perform triage.
“It’s more efficient to have one doctor at the front, meeting ambulances and ordering the appropriate tests,’’ he said.
With an average ER wait of 42 minutes, Lawrence & Memorial in New London also places a doctor in triage to shorten waits, said Dr. Oliver Mayorga, L & M’s chairman of emergency medicine.
“This also improves the quality of care because it puts the most experienced set of eyes out there seeing patients right away,” he said.
Posting Times
In 2009, Middlesex began posting its ER waiting times on a website, which now has 36,000 direct hits a year, spokeswoman Peg Arico said.
Dr. Jonathan E. Bankoff, medical director of Middlesex’s emergency department, said it’s one way for ERs to market their services.
“We welcome, if you will, a bit of friendly competition,” he said.
Windham, The Hospital of Central Connecticut, Johnson Memorial Hospital in Stafford and St. Francis Hospital and Medical Center in Hartford also post ER waiting times on their websites. The Hospital of Central Connecticut also has an iPhone app for patients to check waiting times, and St. Francis even lets patients “check in” to the ER through its website.
Stamford’s Podber said one downside to posting times is that it can give patients a false expectation.
“It’s not like you’re taking a number at the deli,” he said.
“People come in who are a higher priority and need to be seen more quickly and that gets lost.
Bpt hospital is a few hours wait I wait# 7 hrs one time
As a 17 year EMT, there are several things that should be clarified in this article:
1) How are wait times measured?
Is it the moment a patient walks through the door? From when they are triaged (which can take 5-15 minutes)? Registered? Moved into a cubicle and seen by a nurse? Or doctor?
2) Several hospitals have begun registering their patients before a nurse can triage them. Finding a registration clerk can sometimes result in a delay in care. This is a relatively new thing and I don’t understand why they do it – probably for better tracking of resources, cost containment, or maybe to comply with a new Obamacare regulation?
3) The article suggests that patients brought in by ambulance ALWAYS are seen first. NOT TRUE!!!!
In fact, this has been a very mistaken notion we deal with every day. It is NOT APPROPRIATE that patients brought in by ambulance are necessarily seen first unless of course they need to be.
Every day, the ambulance and 911 system is abused by patients, nursing homes and families that call for a relatively routine problem. You’d be surprised at how often these patients can walk on their own, brought in by ambulance and their families follow the ambulance in their own vehicle. Many believe they will circumvent long wait times because they come in by ambulance.
Patients with low acuity are often placed back in the waiting room, or perhaps a bed just inside the door and will wait just as long as if they had walked in on their own. Yet, this still results in delays for crews to get their gear back together while dispatchers are calling them for the next 911 call.
Of course, with severe – or questionable conditions should call 911. Ambulance personnel can radio ahead to have appropriate staff standing by when they arrive. Chest pain, difficulty breathing, symptoms of strokes (sudden headache, numbness, weakness on one side, slurred speech, blurred vision and other neurological symptoms), severe pain, bleeding, trauma, etc. should always call 911. Anyone who cannot ambulate should call for an ambulance as well. For instance, severe debilitating back pain is a condition that many patients apologize for, yet ambulance personnel are specially trained to assist with.
4) Why do patients use the ER on such a frequent basis?
It would nice to do a survey on why the ER is used as opposed to another appropriate medical resource. And I think the results would be surprising and not necessarily the stereotypical reasons that many may think. Sometimes other facilities are not open after hours or on weekends or a patient can’t get a quick enough appointment. Often, chronic conditions pop up. Extended Care Facilities (nursing homes) comprise a very large percentage of all ambulance calls.
It would be interesting to see -either at intake or discharge -to see if a more appropriate setting could have been used for some of these patients if the consumers knew about them, or such resources were available. Of course, the fear of doing such a survey could bring on the concern that these reasons would be denied by an insurance company when the purpose is only to improve the healthcare system as a whole.